total Hip replacement
Total hip replacement is a very successful
operation for relief of pain and improved
mobility. Over 52,000 total hip
replacements were performed in the nhs
and 23,000 in private hospitals in 2010.
Total hip replacement is a safe operation,
but does have some relatively small risks.
Commonly quoted risks include infection,
bleeding, nerve damage, dislocation, leg length discrepancy, loosening, failure & revision, DVT/PE(blood clots), strokes, heart attacks, death.
It is important you discuss your level of risk ,and the implications, with your surgeon.
implants
There are hundreds of different types of hip replacement
prostheses. It is important to chose a joint replacement
with a long history of survivorship to ensure the best
outcome (ODEP rating).
The National Institute of Clinical Excellence (NICE) has published a benchmark for all implanted hip replacements. Each implant must have a rate of revision for failure of 10% or less at 10 years. The Orthopaedic Data Evaluation Panel (ODEP) provides a rating for implants based on their history and survivorship.
Hip replacements can be cemented, un-cemented or a combination (Hybrid). At Torbay Hip Clinic we use the Exeter/ Contemporary cemented system or the Corail/Pinnacle un-cemented System. Both have a long survivorship and one of highest ODEP ratings.
CEMENTED:
The Exeter hip was first implanted in 1969 and is one of the most successful cemented hip implants to date. The stem is held in place with cement (polymethylmethacrylate). The stem itself acts like a wedge which pushes into the cement for a tight fit. A plastic hip socket is usually cemented in place.
UN-CEMENTED:
The Corail/Pinnacle un-cemented hip replacement is the most successful un-cemented hip system in Europe. It was designed 25 years ago. The implant is coated with hydroxyapetite(synthetic bone) and the patient’s bone grows onto the implant over time. When we exercise this results in micro-fractures to our bones. This is normal and our bone repairs itself. This is why our bone becomes thicker and stronger when we exercise more. One of the potential advantages of un-cemented implants is the ability for this process to continue to ensure good fixation of the implant. This process does not occur with cemented implants and as a result in younger active patients cemented implants can loosen and require revision.
HYBRID:
In older more active patients another option is to use an
un-cemented socket(Pinnacle) with a cemented femoral
stem(Exeter). The survivorship of cemented stems is
significantly better than cemented sockets. Also, using
an un-cemented socket allows the surgeon the option of
changing the bearing surface of the hip replacement.
bearing surfaces
There are a choice of different bearing surfaces to form the new hip joint. Traditional hip replacements use metal(cobalt chromium) on plastic sockets. This a typical engineering hard on soft bearing which works very well, but inevitably the soft bearing (plastic socket) wears out if the patient is very active. The plastic wear particles can then lead to loosening of the hip joint in time. Other bearing surfaces have been researched over the years including metal on metal, ceramic on plastic and ceramic on ceramic. Each surface has advantages and potential disadvantages, but modern materials have improved and reduced the risks significantly.
Ceramic on plastic articulations have better wear charactoristics than metal on plastic, but the surgeon is limited to smaller head sizes to maintain good wear properties. Modern manufacturing techniques have produced new plastics with potentially improved wear properties( ultra highly crosslinked). Early research seems to support their use, but there is no long term research currently.
Metal on metal articulations have better wear properties and the advantage of larger head sizes, but the disadvantage is potential metal ion issues. Using large head sizes and ensuring good component positioning reduces the risk of metal ion problems.
Ceramic on ceramic articulations have the best wear properties and you are able to use larger head sizes. Historically, there have been patients where the ceramic has fractured. This was mainly with smaller head sizes. Modern ceramics are significantly stronger and this is unlikely now. Other cases have reported squeaking. This is thought to be related to poor positioning.
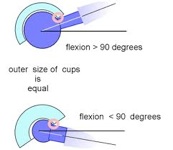
why is femoral head size important?
Dislocation is a potential risk of total hip replacement and resurfacing. This occurs when the head (ball) comes out of the socket. The risk of this is greatest in the first 6 weeks and it generally reduces as time progresses. You can reduce this risk by following the guidance from your physiotherapist. The risk of dislocation is 1-2 per 100 cases. This risk is lower in patients with hip resurfacing or larger head sizes in hip replacement. This is because the ball has a greater distance to lift out of the socket and, with hip replacements, because the neck of the implant is small. Once the hip has dislocated once there is potential for it to keep dislocating and if this occurred a further operation would be needed to correct this.
If a patient has a hard on soft bearing (metal/ceramic on plastic), the wear properties and lubrication are better with smaller head sizes. So the hip would last longer than if a larger head size was used.
If a patient has a hard on hard bearing (metal on metal/ ceramic on ceramic) the lubrication is better with larger head sizes.
Accurate positioning of implants.
Most routine hip replacements can be implanted relatively accurately, but occasionally a patient may have unusual anatomy. Computer Aided Surgery has been demonstrated to improve precision and accuracy with joint replacement surgery. It may be used to optimise implant position and reduce the incidence of poorly positioned implants. This may affect the length of time an implant lasts. Less than 1% of surgeons use Computer Aided Navigation in hip replacement surgery.
Further information on hip replacement precautions and other hip problems can be found here
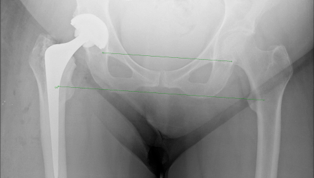
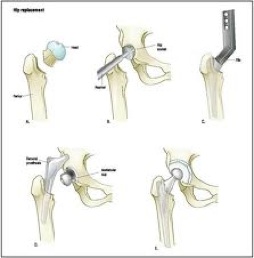
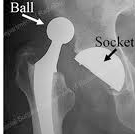
the operation
The x-rays below show what cemented, un-cemented and hybrid hip replacements look like.You can also see how the surgeon can measure the patients leg length post operatively on the hybrid x-ray.