hip resurfacing
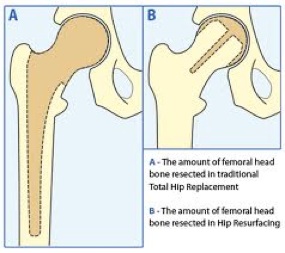
The first hip resurfacing was implanted in 1991. It was designed for younger more active patients by Mr Derek McMinn at the Royal Orthopaedic Hospital, Birmingham. It is a more complex procedure compared to a routine hip replacement and should be performed by a specialist hip surgeon. It involves replacing the ball of the hip joint without placing a long stem down the centre of the femur ( like a traditional hip replacement).
When joint replacements are performed in younger more active patients they generally wear out faster than in older people; just like any mechanical component on a car. This means that younger patients are more likely to require a further hip replacement or revision operation.
There are a number of advantages of hip resurfacing. Patients tend to rehabilitate and recover faster compared to routine hip replacement patients. They also generally return to a higher activity level. Hip Resurfacing preserves more bone in the femur for future replacement operations. It has a metal on metal bearing surface which has excellent wear properties compared to traditional hip replacements. The large femoral head size has been reported to reduce the risk of dislocation.
Patients who have hip resurfacing performed have some risks that traditional hip replacement patients do not have.
1.Femoral Neck Fracture 2-3:100
2.Metal ions complications. 9:1000 risk
These risks mean that a higher early failure rate is recorded in the national joint registry.
The reason for this is partly due to the lower average age of hip resurfacing patients, their high activity levels together with potential weakness in the femoral neck bone. Early failure usually occurs within 1 year and is predominantly caused by femoral neck fracture. If femoral neck fracture occurs it is usually not difficult to revise to a traditional hip replacement.
A small number of patients can have problems with high levels of metal ions in the tissues which may cause failure of the resurfacing. This has been highlighted recently in the media with concerns regarding the particularly high failure rate of the ASR hip resurfacing component. Research has shown that the brand, size, and sex of the patient together with position of the implant may affect the amount of metal ion production. Correct positioning is paramount, and for this reason Mr Higgins feels that computer aided navigation is a valuable tool.
In view of the recent concerns regarding metal on metal implants we follow all our hip resurfacing patients up annually with an x-ray and clinical assessment to ensure that any issues can be identified early. We perform metal ion levels or scan patients if there are any concerns as recommended by the British Hip Society.
Further patient information including patient experiences can be found at www.surfacehippy.info
what is it?


Rehabilitation Exercise Regime post Hip Resurfacing.
Courtesy of the McMinn Centre, Birmingham