Total knee replacement
WHEN SHOULD I CONSIDER IT?



Osteoarthritis is the commonest reason to consider a total knee replacement. Various conditions/problems can lead to osteoarthritis including rheumatoid arthritis, previous fractures or ligament injuries and infections. The indications for total knee replacement are pain, and loss of mobility supported by x-ray changes.
The osteoarthritis may affect different parts of the knee joint. There are 3 main compartments in the knee joint.
-
1.Patello-femoral (Under the knee cap)
-
2.Medial Tibio-femoral (Inside of knee)
-
3.Lateral Tibio-femoral (Outside of knee)
If your arthritis involves two or more of these compartments and you have pain with reduced mobility then a Total Knee Replacement may improve your quality of life.
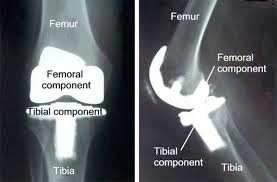
The x-ray above shows reduced joint space between the tibia and the femur in the medial tibio-femoral compartment.
WHAT DOES THE X-RAY SHOW?
When a surgeon looks at your x-rays he is looking for reduced joint space (thinning of the cartilage covering), extra new bone formation (osteophytes), bone cyst formation and thickening of the bone underneath the joint surface (subchondral sclerosis). These are all radiological signs of osteoarthritis. He will also be looking at the quality of your bone, the alignment of your leg and for any evidence of bone loss in severe deformities.


WHAT DOES THE OPERATION INVOLVE?
Total knee replacement is a commonly performed operation in the United Kingdom. Over 70,000 Total Knee joints are implanted each year and the figure is increasing each year. Over half of the operations are performed in women.
Modern techniques using patient specific instruments or Computer Aided Navigation techniques can improve accuracy compared to traditional techniques. This may improve the length of time the implant lasts for.
The operation involves a straight incision over the knee cap and replacing the cartilage of the knee with metal cap over the femur and tibia. These metal knee components are usually cemented in place and have a plastic liner/ insert in between. Sometime the knee cap also has a plastic cap cemented over it’s joint surface.
The majority of surgeons in the UK do not resurface the patella (knee cap). Instead they interrupt the nerve supply to it preserving the bone and relieving the pain. In a small number of cases patients can still have some discomfort from the knee cap and a resurfacing can be performed at a later stage. The reason for this reluctance to resurface the knee cap is the risk of potential complications including patella fracture and loosening of the component. Patients who suffer from Rheumatoid arthritis usually need to have their patellae resurfaced because the incidence of symptoms is higher.



WHAT ARE THE RISKS?
Total Knee Replacement is a safe operation, but there are potential complications that can occur at any age.
The main risks are infection, bleeding, stiffness, painful scar, numbness around the scar, fracture, failure/revision, DVT/PE (blood clots), heart attack, stroke.
Most patients are happy with their knee replacement and have relief from the majority of their pain. However, some patients still have some mild discomfort. As a result of this the patient satisfaction after Total Knee Replacement is not as high as after Total Hip Replacement. (Approximately 95-8% of people are very happy with THR, compared to 70% of TKR patients)